

Public Health TTX - Road to Crisis
The Road to Crisis in Eastern Democratic Republic of the Congo
Overview
The Democratic Republic of the Congo (DRC) is approximately 2.345 million square kilometers (905,000 square miles), making it roughly one quarter the size of the United States (including Alaska). Because it lies on the equator, map projections tend to make it look smaller. Figures 1 and 2 show a political map of the DRC and a zoomed-in view of the area of focus for the exercise. The exercise takes place near Goma, in North Kivu state, along the eastern border with Rwanda.
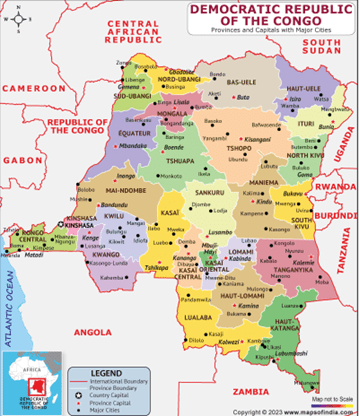
Figure 1. Political Map of the DRC with State Borders.
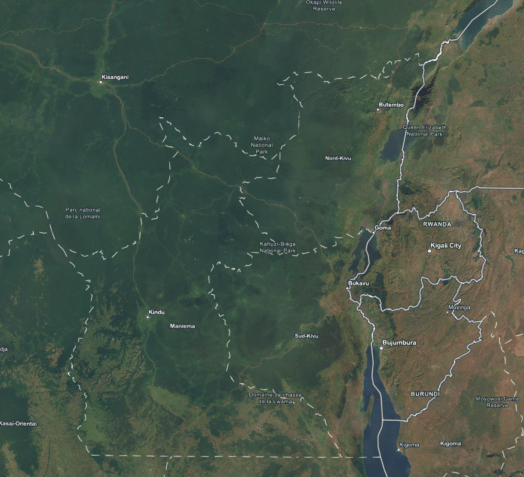
Figure 2. Map focused on Goma, showing location of Camp Rusayp and the Bushagara IDP Camp.
Time of Year: Early May, rainfall has been consistent with frequent flooding. This is the end of the rainy season but still significant rain, which will quickly reduce to less than 1 inch per month for the next three months. Flooding will give way to water shortages.
Overall Country Demographics
Population: 115 million
0-14 years: 45.7% (male 26,584,268/female 26,208,891)
15-64 years: 51.8% (male 29,845,450/female 29,884,958)
65 years and over: 2.5% (2024 est.) (male 1,258,442/female 1,621,018)
Note: At 16.9, DRC has one of the youngest median ages in the world. For comparison, U.S. median age is 38.9
Language
While French is the official language (used in government, education, administration, and much of the media), recent estimates show that only about 51% of the population (roughly 55 million out of 109 million) speaks French. A 2021 survey found that 74% of Congolese report using French as a language of communication (higher among men at 79%), but this often means it functions as a second or third language with varying fluency—many people have only basic or functional skills rather than full conversational or technical proficiency.
Native French speakers make up just ~12% of the population, and proficiency is notably higher in urban centers like Kinshasa (where ~68–69% can speak and understand it) than in rural or eastern regions. In refugee and internally displaced persons (IDP) camp settings—especially in conflict-affected eastern areas—French comprehension drops significantly.
The four national languages (recognized in the constitution) serve as the real lingua francas for everyday life:
- Lingala: Dominant in the west, including Kinshasa and much of the northwest; also widely used in the military, music, and urban settings (second-most spoken overall, used by ~59% in the 2021 survey).
- Swahili (Congo Swahili / Kingwana variant): The primary lingua franca across the east and southeast, including key areas like Goma, Bukavu, and many eastern refugee/IDP camps. It is heavily used in cross-border trade and daily communication.
- Tshiluba (Luba-Kasai or related variants): Common in the central and southern Kasai regions.
- Kituba (Kikongo ya Leta): Used in the southwest and parts of the west.
The DRC has over 200 indigenous languages (mostly Bantu), and multilingualism is the norm—many people speak their ethnic mother tongue + one national language + some French. In humanitarian and public health contexts (such as your tabletop exercise scenarios involving hidden hunger, Ebola/Sudan virus suspects, lactation challenges, or maternal/child health in DRC refugee camps), this linguistic reality creates practical barriers.
For example, in eastern camps near Goma, Swahili is the language most residents rely on for critical information, and public health messaging delivered only in French often fails to reach the majority effectively.
Religion
The Democratic Republic of the Congo (DRC) has one of the highest proportions of Christians in the world. According to the most recent U.S. government estimate drawing on the World Religion Database (2020 data), approximately 95.1% of the population identifies as Christian, 1.5% as Muslim, and 2.5% as unaffiliated or belonging to other small groups.
Detailed breakdown (approximate percentages of total population)
- Christianity: 95.1%
- Roman Catholic: ~47% (nearly half of all Christians)
- Protestant and other Christian groups: ~48% (includes ~60 denominations, evangelicals, and the large Kimbanguist Church—Church of Jesus Christ on Earth through the Prophet Simon Kimbangu—which is an independent African-initiated Christian movement)
- Smaller Christian communities: Jehovah’s Witnesses, The Church of Jesus Christ of Latter-day Saints, Greek and Independent Orthodox Churches.
- Islam: 1.5% (predominantly Sunni; Muslim leaders sometimes estimate higher—up to 5%—when including foreign-born residents from West Africa, but self-identified figures remain low).
- Unaffiliated / Other: 2.5% (includes small numbers of Hindus, Baha’is, Buddhists, Jews, and followers of Indigenous religions).
Important context on older data and everyday practice The last national census (2012) reported roughly 55% Catholic and 32% Protestant (or vice versa depending on the survey), with 2% Muslim and 11% “other.” These figures are still referenced but are now considered outdated given population growth and shifts. Many Congolese practice syncretism—blending Christian beliefs with traditional Indigenous elements such as ancestor veneration, belief in spirits, or kindoki (witchcraft). This is widespread and situational rather than exclusive, so rigid “one religion only” categories can understate cultural realities.
In eastern DRC refugee and IDP camp settings (e.g., around Goma or Bukavu, the focus of many humanitarian scenarios), the national pattern holds: the large Catholic and Protestant networks remain the dominant faith institutions, while traditional beliefs often influence health-seeking behaviors. For your tabletop exercise, this means public-health professionals might realistically encounter scenarios where:
- Faith leaders (priests, pastors, or Kimbanguist elders) are key partners—or gatekeepers—for vaccination drives, nutrition programs, or Ebola/Sudan virus response messaging.
- Families request spiritual explanations or rituals alongside clinical care for issues like hidden hunger, lactation difficulties, or mental health.
- Trust-building requires sensitivity to syncretic practices rather than purely secular or Western medical framing.
Education
The Democratic Republic of the Congo (DRC) has persistently low education levels overall, with notable gender gaps (favoring males), high dropout rates after primary school, and very poor learning outcomes despite some progress in access.
Data come primarily from UNESCO Institute for Statistics (UIS), World Bank/UNESCO reports, and the most recent Demographic and Health Survey (DHS) 2023–24. Note that statistics vary slightly by source and year due to methodological differences (e.g., self-reported literacy vs. tested proficiency, household surveys vs. administrative data), conflict-related data gaps, and rapid population growth. The latest comprehensive breakdowns for the population focus on ages 15–49 (DHS) or school-age groups; full population 15+ data are often modeled or older. Occupation-specific cross-tabs for the entire population are limited and outdated (mostly from labor/employment surveys around 2012).
Literacy Rates
Literacy is defined as the ability to read and write a simple statement (standard UNESCO/DHS definition). Data are strongest for reproductive-age adults (15–49) via DHS, which includes testing or self-reporting.
- DHS 2023–24 (ages 15–49): 59% of women and 86% of men are literate.
- Other/recent estimates (ages 15+): Total adult literacy has been reported around 77–80.5% in recent years (e.g., ~80.5% in 2022), with a clear gender gap (males higher). Youth literacy (ages 15–24) is higher: ~88.1% overall, 85.4% female, 90.8% male (2022).
By age: Younger cohorts (youth 15–24) generally show higher literacy than older adults, reflecting gradual improvements in access over time. Specific older-age breakdowns (e.g., 25–49 vs. 50+) are not detailed in the latest summaries, but overall adult rates lag behind youth.
By gender: Consistent male advantage of 20–27 percentage points (depending on the source/year). This gap narrows somewhat in urban areas and among younger groups but persists nationally.
Educational Attainment (Highest Level Completed or Attended)
DHS 2023–24 provides the most recent population-level data for ages 15–49 (women and men). Exact category breakdowns in available summaries are partial/incomplete in aggregation, but key highlights include:
- No education: 15% of women and 4% of men (ages 15–49).
- Primary-level exposure is limited in the summarized data; many who start primary do not complete it.
- Secondary or higher: Roughly 13% of women and 22% of men reach this level (partial data; actual figures are higher when including incomplete secondary).
Older DHS (2013–14) showed similar patterns but slightly higher secondary/higher attainment for men (~74%). Progress is evident in enrollment but not always in completion.
By age: Attainment improves in younger cohorts due to expanded access since the 2000s–2010s (e.g., higher secondary exposure among 15–24 vs. older groups), though data are not granular in the latest reports.
By gender: Large gap—women are overrepresented in “no education” and underrepresented in secondary+. Urbanization has helped narrow it somewhat, but rural women lag significantly.
Enrollment, Completion, and Out-of-School Rates (School-Age Population)
These better capture current demographics (children/youth):
- Primary: Gross enrollment has improved, but net attendance/completion remains low. Primary completion rate (2021): ~79% girls, 86% boys (overall ~67–70% in recent years). Out-of-school rate for primary age: ~13–22% (household surveys); modeled estimates ~17–24%. Many children start late or drop out.
- Lower secondary: Sharp drop-off. Completion: 51.4% girls, 63.5% boys (2018–2021 data). Gross secondary enrollment: 44% females vs. 70% males.
- Upper secondary/tertiary: Very low. Upper secondary completion ~25–31% (2013–2018). Tertiary gross enrollment: 5% women, 8% men (2020).
- Pre-primary/early childhood: Extremely low (~4–20% enrollment/attendance).
Gender parity index (GPI): Close to 1.0 or slightly favoring girls at primary in some years, but drops to ~0.7 at upper secondary (girls disadvantaged).
Learning outcomes: Extremely poor. Learning poverty (children ~age 10 unable to read/understand a simple text): ~97%. Only ~3–9% achieve minimum proficiency in math/reading by end of primary (2019).
By Occupation / Employment Status
Detailed cross-tabulations of education level by specific occupation (e.g., % of farmers with secondary education vs. professionals) are not available in recent public national statistics. However:
- Education is a strong predictor of employment type (from 2005–2012 labor/employment data, the latest detailed analysis available): Higher attainment reduces the likelihood of agricultural self-employment (dominant sector, ~70%+ of employment) and increases chances of wage employment (public or non-agricultural private) or non-agricultural self-employment. For example, those with postsecondary education were far more likely to be in stable wage jobs.
- Unemployment is paradoxically higher among the most educated (possibly due to limited formal job absorption and longer job-search capacity), while those with no/primary education are mostly in low-productivity agriculture/informal work.
- Gender intersects here: Women (lower average education) are overrepresented in informal/low-skill agriculture and trade.
In summary, the DRC population’s education profile shows slow improvement in access but deep challenges in retention, quality, equity (especially gender and rural/urban), and relevance to the labor market. Primary education reaches most but is often incomplete and low-quality; secondary and beyond remain elite. Conflict, poverty, child labor, early marriage, and infrastructure gaps drive disparities. For the absolute latest or province-level data, consult the full DHS 2023–24 report or UIS/World Bank databases, as new releases continue.
PMESII-PT
Below is a very brief PMESII-PT (Political, Military, Economic, Social, Information, Infrastructure, Physical Environment, and Time) breakdown of the Democratic Republic of the Congo.
Political
The DRC operates as a centralized presidential republic under President Félix Tshisekedi, but governance remains weak, highly corrupt, and fragmented. Eastern provinces face significant challenges from armed group control (e.g., M23/AFC advances that captured Goma and Bukavu in early 2025–2026), leading to parallel administrations, contested authority, and tensions with neighboring Rwanda/Uganda. Humanitarian access is often negotiated with both government and non-state actors. Public-health coordination requires engaging national Ministry of Health structures alongside local leaders and faith-based organizations, as central policies frequently fail to reach or gain acceptance in conflict zones.
Military
Ongoing high-intensity conflict in the east involves the Congolese Armed Forces (FARDC), numerous armed groups (M23, ADF, FDLR remnants, and others), and reported external support. Violence has driven repeated displacement, attacks on health facilities (dozens documented annually), and protection threats to aid workers. In refugee/IDP settings, military operations can restrict movement, disrupt supply chains for vaccines or nutrition supplements, and create “no-go” zones. Public-health teams must plan for force protection, humanitarian notification protocols, and scenarios where military actors influence (or block) access to camps.
Economic
The economy shows strong macroeconomic growth driven by mining (cobalt, copper, coltan), yet most Congolese live in extreme poverty. Widespread unemployment, inflation, and disrupted livelihoods in the east exacerbate food insecurity (projected 16–27 million people needing assistance in 2026, with Crisis/Emergency IPC phases common among displaced households). In camps, limited cash, destroyed markets, and high emergency spending by the government strain resources. Public-health programming must address “hidden hunger” (micronutrient deficiencies) alongside cash/voucher assistance, as economic coping strategies often include risky behaviors that worsen maternal health or disease transmission.
Social
Population exceeds 110 million, with a very young demographic and high fertility. Society is deeply religious (≈95% Christian—roughly half Catholic, half Protestant/Kimbanguist—with widespread syncretism blending Christian and traditional beliefs). Ethnic diversity (over 200 groups) and strong community/faith networks shape health-seeking behavior. Gender dynamics include high rates of gender-based violence in conflict zones. In refugee scenarios, social factors affect vaccination acceptance, breastfeeding practices, and mental health; faith leaders often serve as critical partners (or gatekeepers) for outreach on cholera, mpox, or nutrition messaging.
Information
Multilingual environment (French official but limited proficiency; Lingala in west, Swahili dominant in east). Information flows through radio, community leaders, churches/mosques, and increasingly mobile phones/social media, though misinformation and distrust of “outsiders” are common. In camps, rumors about vaccines, treatment, or aid distribution can undermine response efforts. Effective public-health communication requires translated, culturally adapted materials (Swahili prioritized in eastern settings) and engagement with trusted local voices rather than top-down French-language campaigns.
Infrastructure
Severely degraded, especially in the east. Many health facilities are non-functional or overwhelmed (e.g., 70% in parts of North Kivu); roads, water/sanitation systems, and electricity are unreliable. IDP camps often lack adequate latrines, clean water, and cold chains for vaccines. Conflict has destroyed or occupied structures, forcing reliance on mobile clinics or makeshift sites. Public-health responses must account for logistical constraints on delivering therapeutics, therapeutic foods for malnutrition, or maternal care kits.
Physical Environment
Vast, biodiverse country with dense equatorial rainforests, volcanic highlands in the east (around Goma), rivers, and flood-prone lowlands. Tropical climate drives vector-borne diseases (malaria, yellow fever) and waterborne outbreaks (cholera). Displacement into overcrowded camps or flooded areas heightens risks of acute malnutrition, respiratory infections, and rapid disease spread. Seasonal rains and poor drainage complicate camp management and WASH interventions.
Time
Conflict and displacement are protracted (decades-long), with acute escalations creating rapid-onset needs (e.g., new waves of IDPs/returnees in 2025–2026). Seasonal factors include harvest cycles affecting food stocks (lean season peaks) and rainy/dry seasons influencing disease transmission. Public-health timelines are compressed by funding shortfalls, election/political cycles, and humanitarian access windows. Exercises should stress “golden hours” for outbreak containment and the cumulative fatigue of repeated displacements on community resilience.
Road to Crisis
April saw heavy flooding in the entire region. This has had cascading effects on the population, including food shortages, difficulty accessing medical care, and instances of cholera. Many medical facilities were damaged by the floods. Militant factions and criminal gangs took advantage of the instability. In Kirotshe, North Kivu, nearly all health infrastructures have been destroyed or looted, with 29 out of 31 health centers left inoperable. Flooded roads combined with the security situation has made resupply intermittent.
The March 23 Movement, known as M23, is a prominent armed group in the region. There is evidence of direct foreign support, notably from Rwanda. M23 resurged in 2025 and occupies several towns in North- and South-Kivu. Publicly available information suggests that M23 continues to actively recruit and train militants. Several atrocities have been attributed to M23.
- As the floods taper, relief workers can once again take stock of the situation, which is critical:
- Basic medical supplies are running short, including things like nitrile gloves and gowns
- Some medical equipment, such as x-ray machines, EEGs, etc., has been damaged or destroyed
- Certain medical records are missing, were destroyed, or were not kept properly during the last 90 days.
- Many medications are critically low
Your Role
A cluster of two refugee camps exists near Goma. You are from a UN-sponsored non-governmental organization (NGO) tasked to manage the health situation of the camps. (Note: The camps are/were real camps but information regarding them is notional).
Camp Rusayo: https://maps.app.goo.gl/uU62qFWhFkg7f78v9
Last reported population: 25,931
Current estimate: 18,500
Bushagara IDP Camp: https://maps.app.goo.gl/vJtRpXeALKtyDZaW9
Last reported population: Approx 22,000
Current estimate: 12,000
Figure 3 shows a picture of Camp Rusayo from 2024.

Figure 3. Camp Rusayo.
Though the camps share an administrative structure, there is a complex system in place for the management of healthcare. This is based on support provided by several NGOs and oversight from the UN and WHO. The varying degrees of support and expertise has led to an ad hoc system. There is also physical danger outside of the camps, making the movement of patients or medical personnel dangerous.